

3 minute read
Integrated healthcare is most important for communities with limited access to medical and/or behavioral health services. By making those services available in one place and training a care team to collaborate, vulnerable patients are more likely to get the right treatment at the right time. According to a new report, integration makes even more sense for rural communities.
Consider some of these recent trends from the National Healthcare Quality and Disparities Report:
- About 20% of the US population lives in rural or nonmetropolitan areas, although about 85% of the total U.S. land area is classified as rural
- Compared with urban counties, rural counties have:
- A larger percentage of adults over the age of 65 (17.5% vs. 13.8%)
- A higher poverty rate (15.3% vs. 11.9%) and lower per capita income ($42,993 vs. $59,693)
- A smaller percentage of adults who get enough physical activity (20% vs. 25%)
- A higher prevalence of adults with multiple chronic health conditions (e.g., arthritis, diabetes) (34.8% vs. 26.1%)
- In 1999, the age-adjusted death rate in rural areas was 7% higher than in urban areas; by 2019, the rate in rural areas was 20% higher than in urban areas
- Rural areas make up the majority of all HRSA-designated health professional shortage areas
- From January 1, 2010, to September 2021, 138 rural hospitals closed
In November 2021, the Agency for Healthcare Research and Quality (AHRQ) published the “Chartbook on Rural Healthcare”. This publication is full of essential information for managers, policy makers, and executives serving rural areas.
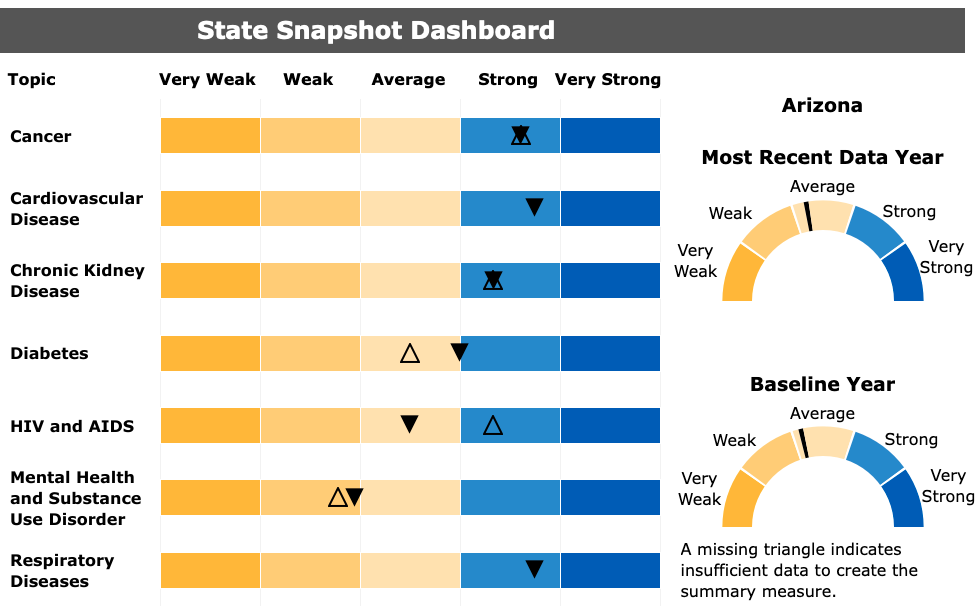
Specifically, it includes a summary of trends in healthcare quality and disparities for rural populations and figures showing measures of healthcare access and priority areas (e.g., patient safety, care coordination, etc.). There is an online dashboard you can use to look at a snapshot of your own state.
I used the dashboard to look at Arizona, where I live. My state is average on priority areas and access to care. We are strong on specific health diseases like cancer, cardiovascular disease, chronic kidney disease, and respiratory diseases. We are weak on mental health and substance use disorders and very weak on care for elderly adults. The dashboard lets me compare baseline performance (year varies) to recent performance.
Think about how to use this information. Often a manager or care team will have anecdotal information pushing them to offer a new service or improve an existing one. Perhaps a clinician suggests investment in a mobile clinic unit or a patient advocacy panel recommends hiring more social workers. Good ideas, but hard to know if they are the right ones.
Using empirical data, like this AHRQ report, allows a clinic to match the right solution to the right problem. For example, in my state of Arizona, this report shows that we have worse than average performance on treating mental health and substance use. I can use that information to apply for new funding and improve access in key areas. Data are the currency of the kingdom, so to speak, and open doors for more precise solutions.
Leave a Reply