

5 minute read
Several years ago, I did an audit of PHQ-9 scores in our clinic and noticed that the total scores did not always match the individual item scores. Nurse, I need a calculator, stat.
At the time, my team took a universal, paper-based screening approach for depression: patient answers questions on a clipboard; medical assistant calculates and records the score; provider gets notified. Pretty straightforward. My own math skills notwithstanding, this exposé of my team’s math skills revealed an opportunity to remove the risk of human error and expand our behavioral health screening capacity.
Using Adobe Captivate, I designed a digital survey with scoring technology and pre-screening questions for several behavioral health needs: depression, anxiety, alcohol use, drug use, suicide risk, and bipolar disorder. The scoring algorithm decided when patients qualified for a full screening based on their pre-screen answers.
After working out the IT stuff, we now had an automated behavioral health survey on tablets. Unfortunately, the tablet could not “talk” to the health record system, so the medical assistants recorded the scores. After a successful pilot run, we began using the tablets for all new patient appointments.
Visions of new questions and measures began to dance in my head. What about ACEs? What about health literacy? What about unsafe sexual behaviors? Pediatric screening measures? Be still, my beating heart.
Clearly, I was intoxicated with the vision of amassing untold data points from our patients with no clear plan of what to do with the data. I was like Benjamin Franklin flying my kite in a thunderstorm, but with no follow-up plan for harnessing electricity once lightning struck.
Upon Further Reflection
Sometime later, I reflected on this experience. First, I started with what I knew to be true.
Primary care is a great place to deliver and coordinate healthcare services that are timely and effective. Check.
Screening in primary care is pretty common and functions as a preventive measure for identifying patients with undetected health problems. Yes, most definitely.
Although integration has made a difference, behavioral health screening is fairly uncommon. Bingo. That is what brings us together today.
Scientific evidence shows that we should screen for all behavioral health conditions known to humankind. Stop the press. Pump the brakes. Slow down there, Benji. Is this true? Not 100% sure. So, I checked it out.
USPSTF Recommendations
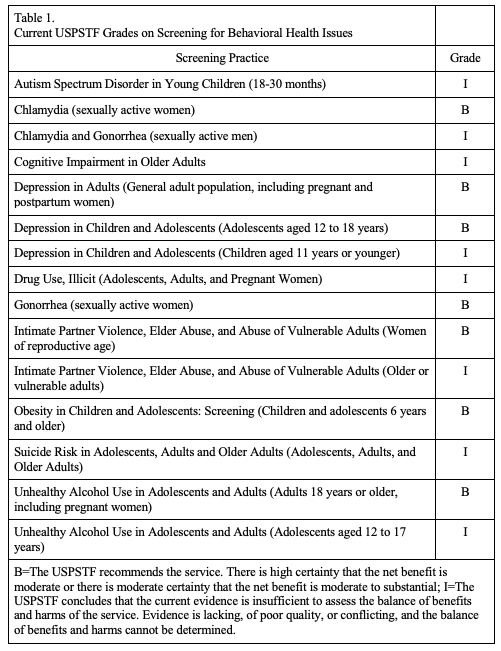
To answer this question on the evidence behind behavioral health screening in primary care, I turned to the US Preventive Services Task Force (USPSTF), which plays an important role in reviewing, critiquing, and summarizing the evidence for preventive care approaches like screening. To date, USPSTF has issued recommendations on multiple screening practices related to behavioral health [1] (see Table 1 attachment below).
According to the USPSTF, screening is recommended for chlamydia and gonorrhea (women only), depression in adults and adolescents 12-18, violence or abuse toward women of reproductive age, and unhealthy alcohol use in adults.
Screening is not recommended for autism spectrum disorder, chlamydia and gonorrhea (men only), cognitive impairment in older adults, depression in children, illicit drug use, violence or abuse toward older or vulnerable adults, suicide risk, and unhealthy alcohol use in adolescents 12-17. Screening is not recommended when evidence is lacking, of poor quality, conflicting, or the balance of benefits, and harms cannot be determined. USPSTF strongly recommends only screening when follow-up monitoring and treatment is available.
Further, USPSTF evaluations are limited to single-condition screenings and do not include comorbidities, lifestyle (except obesity in children and adolescents), and strategies peripheral to screening (e.g., screening frequency, medium, interpretation, documentation, etc.).
Based on these findings, I realized the current literature does not support screening for all conditions under the sun. I knew that intuitively, but it was affirming to see it from a reputable source. I also knew, after implementing our tablet-based survey in the clinic workflow, that screening can also lead to false and soft positives, the former being a result of human error and the latter a sign that the patient is not ready for services. These positives clogged our referral pipeline, preventing patients with more acute needs to receive services.
I also realized that our current screening technology needs more sophistication. We need more measures that go beyond single-disease symptoms and a better understanding of optimal timing. We also need to figure out how to easily send data across networks for quick sharing and documentation.
Screening Technology
Here are a few ideas push the field along:
Conduct more effectiveness research to see how quality of life measures perform compared to more traditional measures of disease symptomatology.
Conduct more implementation research to see what factors contribute to screening workflows being feasible, sustainable, and adaptable.
Identify effective strategies peripheral to screening (screening frequency, medium, interpretation, documentation), but important for comprehensive care
Explore strategies for collecting and integrating non-clinical data into clinical decision-making pathways
Two final thoughts for you here. First, we live in a world of limited resources and cannot always treat behavioral health needs on demand. Perhaps one solution then is to focus our screening efforts on people at risk for behavioral health needs and other complications. [2] Second, data is the currency of the healthcare kingdom, if not the entire world. But our current screening technology still feels like the stone age. Integration will continue to improve healthcare systems, especially as we accelerate the development and adoption of better ways to detect our patient’s behavioral health needs in the right place and at the right time.
{kind=link}
1. US Preventive Services Task Force [Internet]. Rockville, MD: Recommendation Topics [cited 2020 June 1]. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation-topics
2. Kathol, R. G., deGruy, F., & Rollman, B. L. (2014). Value-based financially sustainable behavioral health components in patient-centered medical homes. The Annals of Family Medicine, 12(2), 172-175.
Matt,
Really enjoyed this piece. Love the Benji perspective. I still struggle with the frequency of screening and optimizing the timing of screening as well. In an ideal world, regardless of the mechanics of screening infrastructure, integrated care can still reach folks – through effective team-based communication and strategies and provider ability to pick up on issues. However, in a healthcare world where completion of tasks drown out some of the focus and attention of our colleagues due to system / policy / incentive demands, a screener can serve as a way to receive attention to things that may otherwise go untouched.
Deepu, thank you for the comment. Screening is a necessary technology in a system where our attention is a precious and limited resource. Most medical clinicians have little training in how to interview patients for behavioral health problems. A brief measurement tool makes up the difference with limited attention and training to identify patients with unmet behavioral health needs. I’ve learned that screening tools should be carefully chosen and be part of a team-based, effective care pathway.